
Radial Head Fracture
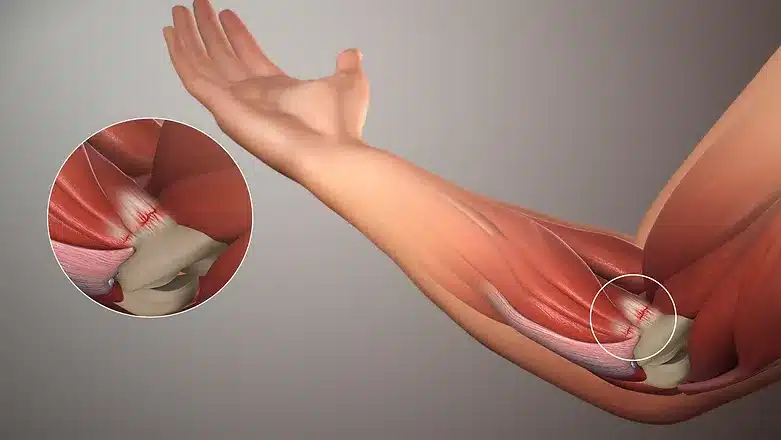
While trying to break a fall with your hands may seem instinctive, the force of the fall could travel up your forearm bones and dislocate your elbow. It also could break the smaller bone (radius) in your forearm. Fractures of the radius often occur in the part of the bone near the elbow, called the radial “head.”
Radial head fractures are common injuries, occurring in about 20% of all acute elbow injuries. Many elbow dislocations also involve fractures of the radial head.
Radial head fractures are more frequent in women than in men, and are more likely to happen in people who are between 30 and 40 years of age.
ELBOW ANATOMY

DISEASE EXPLAINED
SYMPTOMS
Pain on the outside of the elbow
Swelling in the elbow joint
Difficulty in bending or straightening the elbow accompanied by pain
Inability or difficulty in turning the forearm (palm up to palm down or vice versa)
CAUSES
Except for congenital radial head dislocations, which by definition are not acquired, radial head fractures and dislocations are the result of trauma, usually from a fall on the outstretched arm with the force of impact transmitted up the hand through the wrist and forearm to the radial head, which is forced into the capitellum.
Recognizing a congenital radial head dislocation (see the image below), in which the radial head is larger and rounder than expected, is important because operative treatment to reduce a congenital radial head dislocation is not indicated.
TREATMENT OPTIONS
TREATMENT OPTIONS
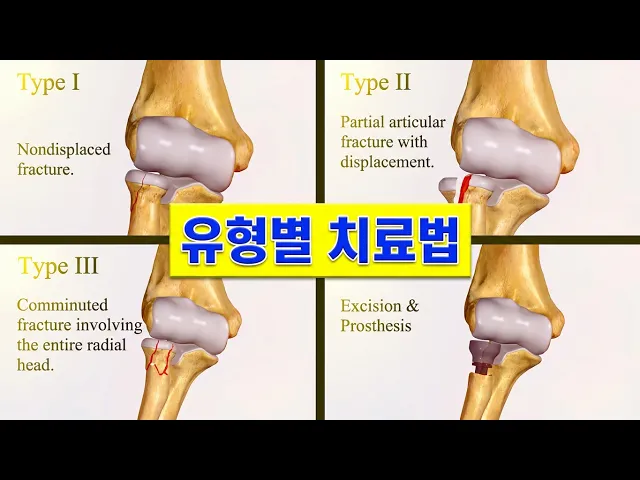
Doctors classify fractures according to the degree of displacement (how far out of normal position the bones are). Treatment is determined by the type of fracture, according to the classification below.
Type I Fractures
Type I fractures are generally small, like cracks, and the bone pieces remain fitted together.
The fracture may not be visible on initial x-rays, but can usually be seen if the x-ray is taken 3 weeks after the injury.
Nonsurgical treatment involves using a splint or sling for a few days, followed by an early and gradual increase in elbow and wrist movement (depending on the level of pain).
If too much motion is attempted too quickly, the bones may shift and become displaced.
Type II Fractures
Type II fractures are slightly displaced and involve a larger piece of bone.
If displacement is minimal, a sling or splint may be used for 1 to 2 weeks, followed by range-of-motion exercises.
Small fragments of broken bone may be surgically removed if they prevent normal elbow movement or could cause long-term problems with the elbow.
If a fragment is large and out of place enough, the orthopedic surgeon will first attempt to hold the bones together with screws, or a plate and screws. If this is not possible, the surgeon will remove the broken pieces of the radial head.
The surgeon will also correct any other soft-tissue injury, such as a torn ligament.
Type III Fractures
Type III fractures have multiple broken pieces of bone which cannot be put back together for healing.
In most Type III radial head fractures, there is also significant damage to the elbow joint and the ligaments that surround the elbow.
Surgery is always required to either fix or remove the broken pieces of bone and repair the soft-tissue damage. If the damage is severe, the entire radial head may need to be removed. In some cases, an artificial radial head may be placed to improve long-term function.
Early movement to stretch and bend the elbow is necessary to avoid stiffness.
Even the simplest of fractures may result in some loss of movement in the elbow. Regardless of the type of fracture or the treatment used, exercises to restore movement and strength will be needed before resuming full activities.
CONTACTING DR. PERLMUTTER
Texting is preferred by Dr. Perlmutter for communication (717-836-6833). Please contact him ASAP, should you have any concerns whatsoever. Many patients fail to contact Dr. Perlmutter when they should have because they are "afraid of bothering him." This is a potentially dangerous attitude and Dr. Perlmutter will always welcome every opportunity to make his patients feel more comfortable. Please feel comfortable sending photographs to add perspective to your questions. Please turn on your flash, aim directly at the body part that you wish to show, and use an evenly colored, dark, and non-reflective background.
If you cannot text, you may call Dr. Perlmutter, however, you must use a confirmed caller ID unblocked telephone or he will not be able to return your call. If you need help turning off this feature you may:
1) Try pushing *82 prior to dialing, or
2) Use a different phone.
Your failure to do so will absolutely compromise your care and hurt your outcome!
If Dr. Perlmutter cannot be reached on his cell phone or by text, please contact the hospital operator to assist in reaching him or a member of his team. They can be reached at NASH: 252-962-8000. ECU Edgecombe: 252-641-7700.
IF YOU PERCEIVE AN EMERGENCY, PLEASE CALL 911 OR GO TO THE EMERGENCY ROOM ASAP.
DISCLAIMER
- All of the opinions expressed within the educational information delivered within the provided links are those of their authors and not necessarily those of either your treating doctor or CRO.
- This site is for educational purposes only!!
- Copyright Disclaimer under Section 107 of the copyright act 1976, allowance is made for fair use for purposes such as criticism, comment, news reporting, scholarship, and research. Fair use is a use permitted by copyright statutes that might otherwise be infringing. Non-profit, educational, or personal use tips the balance in favor of fair use.