
Finger Deformities
Swan-neck deformity
This is a deformity bending in (flexion) of the base of the finger, a straightening out (extension) of the middle joint, and a bending in (flexion) of the outermost joint. The most common cause of swan-neck deformity is rheumatoid arthritis.
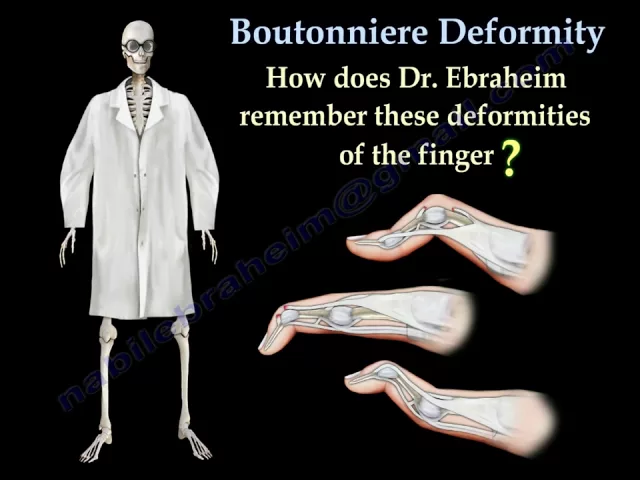
Boutonniere deformity
This describes a medical condition in which the finger is flexed at the proximal interphalangeal joint (PIP) and hyperextended at the distal interphalangeal joint (DIP). This is usually a result of trauma in the acute setting and is caused by a rupture of the PIP central slip.
Mallet finger deformity
A mallet finger is a deformity of the finger caused when the tendon that straightens your finger (the extensor tendon) is damaged. When a ball or other object strikes the tip of the finger or thumb and forcibly bends it, the force tears the tendon that straightens the finger.
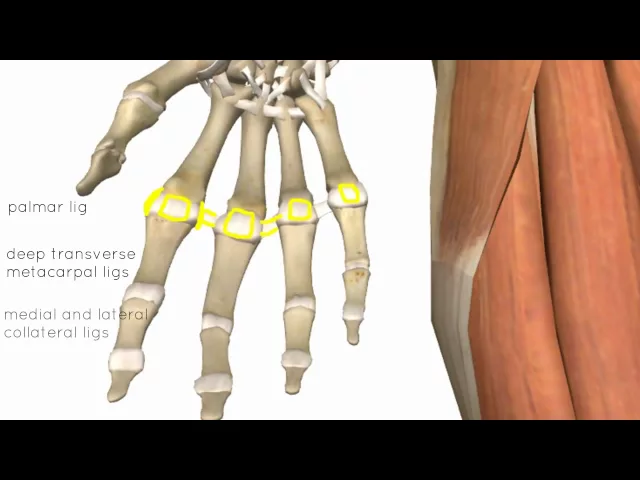
HAND & WRIST ANATOMY
DISEASE EXPLAINED
SYMPTOMS
Swan-neck deformity
Earlier signs of swan neck deformity may include pain when bending the knuckle and a slight bend in the wrong direction of one or more fingers.
In later stages of swan neck deformity, it is relatively easy to recognize symptoms visually.
If it is left untreated, the two outer joints of the finger will eventually bend noticeably, causing the finger to resemble a swan’s neck.
Boutonniere deformity
Signs of boutonnière deformity can develop immediately following an injury to the finger or may develop in a week to 3 weeks later.
The finger at the middle joint cannot be straightened and the fingertip cannot be bent.
Swelling and pain occur and continue on the top of the middle joint of the finger.
Mallet finger deformity
In a mallet finger, the fingertip droops. It cannot straighten on its own power. The finger may be painful, swollen and bruised, especially if there is an associated fracture, but often the only finding is the inability to straighten the tip.
Occasionally, blood collects beneath the nail. The nail can even become detached from beneath the skin fold at the base of the nail.
CAUSES
Causes for Swan-neck deformity includes:
Other types of arthritis
Untreated mallet finger – a condition often caused by injury
Poorly healed fracture in the finger
Other direct trauma to finger that has weakened the ligaments surrounding the proximal interphalangeal joint
Nerve damage that causes muscle spasms
Severely jammed finger tip
Tightened hand muscles due to injury
Looseness of the fibrous plate inside the hand located at the base of the fingers
Loose finger ligaments
Ruptured finger tendon or tendons
Some genetic conditions, such as Ehlers-Danlos Syndrome
Causes for Boutonniere deformity
Boutonnière deformity is generally caused by a forceful blow to the top (dorsal) side of a bent (flexed) middle joint of a finger.
It also can be caused by a cut on the top of the finger, which can sever the central slip (tendon) from its attachment to the bone. The tear looks like a buttonhole (“boutonnière” in French). In some cases, the bone actually can pop through the opening.
Boutonnière deformities may also be caused by arthritis.
Causes for Mallet finger deformity
The most common cause is when the tip of a finger is forcibly flexed or hit against a solid object, such as a ball. This causes the tendon to be torn and unable to fully extend the top of the finger or thumb.
TREATMENT

TREATMENT OPTIONS
Swan-neck deformity
Non-Surgical Treatments
Non-surgical treatment focuses on restoring flexibility to the PIP joint and aligning the hand and fingers. Fixing the PIP joint should fix the DIP joint in most situations. If it does not, additional surgery may be required.
In some cases, a person may receive physical or occupational therapy. These treatments use stretching, massage, and joint mobilization to help restore function and alignment of the fingers and hands.
In addition to therapies or as a stand-alone treatment, a doctor may prescribe special finger splints. These produce the best results when the PIP joints are most supple. Many newer styles of splints resemble jewelry and can be discrete or decorative.
A person may take over-the-counter or prescription medicines to help reduce pain and discomfort. A person should consult their doctor before taking any new medications.
Surgical Options
Before surgery, a surgeon may suggest that a person tries some of the non-surgical treatment options for several weeks.
Severe cases of swan neck deformity, as well as those that do not respond to therapies and splints, are the most likely to be recommended for surgery.
There are several surgical options available. Soft tissue surgery, finger joint fusion, and PIP joint arthroplasty are all viable options for treating swan neck deformity.
Soft tissue surgery involves releasing, aligning, and balancing the ligaments around the PIP joint. However, surgery that aims to fix the soft tissue that contributes to swan neck deformity may not be as effective. After surgery, most people will receive physical therapy to aid recovery.
Finger joint fusion involves fusing the DIP joint so that the fingertip will not be able to bend at the DIP joint. Fusing the DIP joint stabilizes the joint, reduces pain, and avoids further deformity. In more severe cases, a surgeon may recommend fusing the PIP joint in a slightly bent position.
Proximal interphalangeal joint arthroplasty involves replacing part or all of the PIP joint in the affected fingers. Both ligament sections around the joint are removed and replaced. Once the new ligaments are in place, the surgeon typically reconstructs some of the soft tissue to help restore movement to the finger.
Boutonniere deformity
Non-surgical Options
Splint
A commercial splint used in treating boutonnière deformity. Splinting helps keep the ends of the tendon from separating during healing.
Exercises
Your doctor may recommend stretching exercises to improve the strength and flexibility in the fingers.
Protection
If you participate in sports, you may have to wear protective splinting or taping for several weeks after the splint is removed.
People with boutonnière deformity caused by arthritis may be treated with oral medications or corticosteroid injections, as well as splinting.
Surgical Options
While nonsurgical treatment of boutonnière deformity is preferred, surgery is an option in certain cases, such as when:
The deformity results from rheumatoid arthritis.
The tendon is severed.
A large bone fragment is displaced from its normal position.
The condition does not improve with splinting.
Surgery can reduce pain and improve functioning, but it may not be able to fully correct the condition and make the finger look normal. If the boutonniere deformity remains untreated for more than 3 weeks, it becomes much more difficult to treat.
Mallet finger deformity
Nonsurgical Treatment
The majority of mallet finger injuries can be treated without surgery. Ice should be applied immediately and the hand should be elevated (fingers toward the ceiling.) Medical attention should be sought within a week after injury. It is especially important to seek immediate attention if there is blood beneath the nail or if the nail is detached. This may be a sign of a nail bed laceration or an open (compound) fracture.
There are many different types of splints/casts for mallet fingers. The goal is to keep the fingertip straight until the tendon heals. Most of the time, a splint will be worn full-time for eight weeks Over the next three to four weeks, most patients gradually begin to wear the splint less frequently. The finger usually regains acceptable function and appearance with this treatment. Nevertheless, it is not unusual to lack some extension at the conclusion of treatment. Your surgeon or hand therapist will instruct you about how to wear the splint and will also show you exercises to maintain motion in the middle joint (the proximal interphalangeal joint) so your finger does not become stiff. Once your mallet finger has healed, your surgeon or hand therapist will teach you exercises to regain motion in the fingertip.
In children, mallet finger injuries may involve the cartilage that controls bone growth. The doctor must carefully evaluate and treat this injury in children so that the finger does not become stunted or deformed.
Surgical Treatment
Surgical repair may be considered when mallet finger injuries have large bone fragments or joint mal-alignment. In these cases, pins, wires or even small screws are used to secure the bone fragment and realign the joint. Surgery may also be considered if splint wear is not feasible or if non-surgical treatment is not successful in restoring adequate finger extension. Surgical treatment of the damaged tendon can include tightening the stretched tendon tissue, using tendon grafts or even fusing the joint straight. Your surgeon will advise you on the best technique in your situation.
CONTACTING DR. PERLMUTTER
Texting is preferred by Dr. Perlmutter for communication (717-836-6833). Please contact him ASAP, should you have any concerns whatsoever. Many patients fail to contact Dr. Perlmutter when they should have because they are "afraid of bothering him." This is a potentially dangerous attitude and Dr. Perlmutter will always welcome every opportunity to make his patients feel more comfortable. Please feel comfortable sending photographs to add perspective to your questions. Please turn on your flash, aim directly at the body part that you wish to show, and use an evenly colored, dark, and non-reflective background.
If you cannot text, you may call Dr. Perlmutter, however, you must use a confirmed caller ID unblocked telephone or he will not be able to return your call. If you need help turning off this feature you may:
1) Try pushing *82 prior to dialing, or
2) Use a different phone.
Your failure to do so will absolutely compromise your care and hurt your outcome!
If Dr. Perlmutter cannot be reached on his cell phone or by text, please contact the hospital operator to assist in reaching him or a member of his team. They can be reached at NASH: 252-962-8000. ECU Edgecombe: 252-641-7700.
IF YOU PERCEIVE AN EMERGENCY, PLEASE CALL 911 OR GO TO THE EMERGENCY ROOM ASAP.
DISCLAIMER
- All of the opinions expressed within the educational information delivered within the provided links are those of their authors and not necessarily those of either your treating doctor or CRO.
- This site is for educational purposes only!!
- Copyright Disclaimer under Section 107 of the copyright act 1976, allowance is made for fair use for purposes such as criticism, comment, news reporting, scholarship, and research. Fair use is a use permitted by copyright statutes that might otherwise be infringing. Non-profit, educational, or personal use tips the balance in favor of fair use.