
Big Toe Arthritis

Osteoarthritis (OA) is the most common type of arthritis. It can affect joints anywhere in the body. When cartilage in the joints wears down, bones become exposed and rub against each other. This causes swelling and pain in the joint and can limit your range of motion.
OA generally starts slowly but usually worsens over time. The base of the big toe, known as the first metatarsophalangeal joint, is a common site for OA.
BIG TOE & FOOT ANATOMY
DISEASE EXPLAINED

SYMPTOMS
Even in the early stages, arthritis in the toe can cause tenderness, achiness, and joint pain. You may also feel achiness or pain in other toes or the arch of your foot as you walk.
Over time, you may even develop a burning sensation, which is a hallmark sign of nerve pain, or neuropathy.
An arthritic toe may ache after long periods of sitting or when you first wake up in the morning. Stiffness and pain is typically a sign of OA after long periods of inactivity or immobility.
Overgrowth of the big toe bone can make it difficult or even impossible to bend your toe.
More specifically, in people with OA, the joint degenerates and a reactive bone process is triggered, such as spurs or ankylosing. The excess bone growth can lead to fusion of the joint and a fixed, or non-bending joint. The result is a stiff toe, which is also called hallux rigidus.
CHANGING APPEARANCE
Arthritis causes inflammation, so you may notice some swelling around the joint of your toe. Damaged cartilage can lead to bones rubbing against each other.
You can have joint space narrowing, or destruction, but minimal pain. There’s a spectrum of symptoms and radiographic findings that can occur.
Your body will attempt to repair this condition by growing more bone. This creates bony protrusions called bone spurs.
You may be unaware of bone spurs until you develop a visible bump or callus on your toe.
As the big toe changes, it can start to push against the other toes, causing the joint at the base of the big toe to become enlarged. This is known as a bunion. Since this joint capsule enlargement isn’t bone, it won’t show up on X-rays.
DIFFICULTY WALKING
Walking can be a problem if you can’t bend your big toe.
If you don’t already have bunions, the imbalance in the way you walk can make them more likely to develop. As you walk, bunions push against your shoes, causing your big toe to push against your other toes. This makes walking painful.
The subsequent rubbing of the outside joint against your shoes can also make walking painful.
Over time, bunions can lead to corns (central core of hard tissue with callus around it), calluses, and hammertoes, which are toes that are bent downward and may cross over each other.
CAUSES
Your risk for OA increases as you age, which is mostly due to wear and tear. Your body may become less able to heal damaged cartilage as you grow older.
You’re more likely to develop OA if you:
Have a family history of it
Have obesity
Have a prior injury to a joint
Hallux rigidus also may occur due to a toe injury or deformity of the foot. Stiffness in the big toe generally begins between the ages of 30 and 60. Earlier age onset of OV usually indicates the condition is genetically induced.
TREATMENT
TREATMENT OPTIONS
HOME TREATMENTS
Over-the-counter (OTC) pain relievers and anti-inflammatories can help lessen pain and swelling. Placing ice packs on the toe can offer temporary relief.
Choosing the right footwear can make a big difference. High heels, tight shoes, and pointy-toed shoes can encourage the formation of bunions.
You may benefit from pad inserts or arch supports to prevent rubbing and to improve comfort.
Always allow plenty of room for your big toe.
Extra weight adds stress to the bones of your feet, so try to pay attention to your diet and get regular exercise. These lifestyle modifications may help you to feel better and to delay the progression, but they may not stop the progression of OA.
OSTEOARTHRITIS TREATMENTS
Your healthcare provider may take an X-ray of your foot to look for bone spurs and to assess the loss of function of the joint. However, X-rays are not always needed to correctly diagnose OA.
Often, finding a good walking or athletic shoe may help. However, if that option doesn’t work, your healthcare provider may also recommend custom-made insoles or shoes that have stiff soles and rocker bottoms.
Your physical therapist or another healthcare provider can show you how to perform stretches and exercises for your feet. In some cases, a splint or brace may be helpful. A walking cane can help you feel more stable.
Compression socks are also available and may help to manage your condition.
Your healthcare provider can inject corticosteroids directly into your joint to help reduce swelling and relieve pain. A single corticosteroid injection can be effective. However, they can be given 3 or 4 times per year.
Your healthcare provider may also recommend OTC medications, such as topical anti-inflammatory gels or lotions. If OTC medications aren’t effective, they may prescribe other medications.
SURGERY
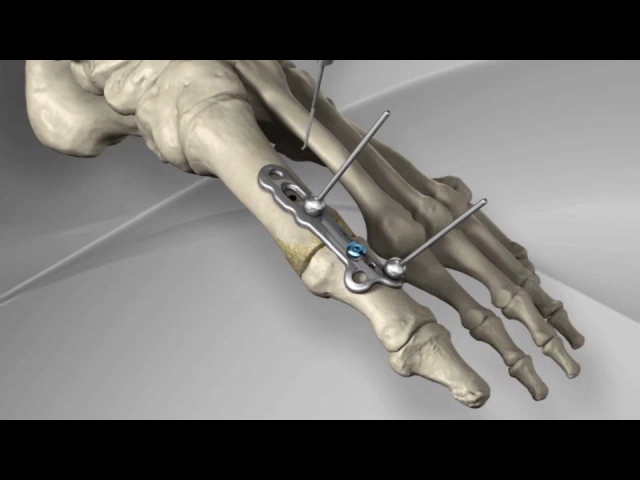
In more severe cases, healthcare providers can surgically remove damaged cartilage and fix the joint in a permanent position, which is called a fusion or arthrodesis. They can do this using a plate and screws, or wires.
Some patients may benefit from joint replacement surgery, which is called an arthroplasty. Surgical options will depend on your activity level and whether your activities require motion of the metatarsophalangeal joint.
Ask your healthcare provider if you’re a good candidate for surgery if nonsurgical treatment doesn’t help.
DISCLAIMER
- All of the opinions expressed within the educational information delivered within the provided links are those of their authors and not necessarily those of either your treating doctor or CRO.
- This site is for educational purposes only!!
- Copyright Disclaimer under Section 107 of the copyright act 1976, allowance is made for fair use for purposes such as criticism, comment, news reporting, scholarship, and research. Fair use is a use permitted by copyright statutes that might otherwise be infringing. Non-profit, educational, or personal use tips the balance in favor of fair use.